You have access to ECG's if you have a surgical monitor with 3 clips that are put on as shown here:

These clips are pretty cool. Even though they are clipped to the skin high up on the pet's legs, they pick up the electrical impulses generated by the heart as it beats and conducts them through wires to the monitor which displays them as a wavy line that should look something like this:

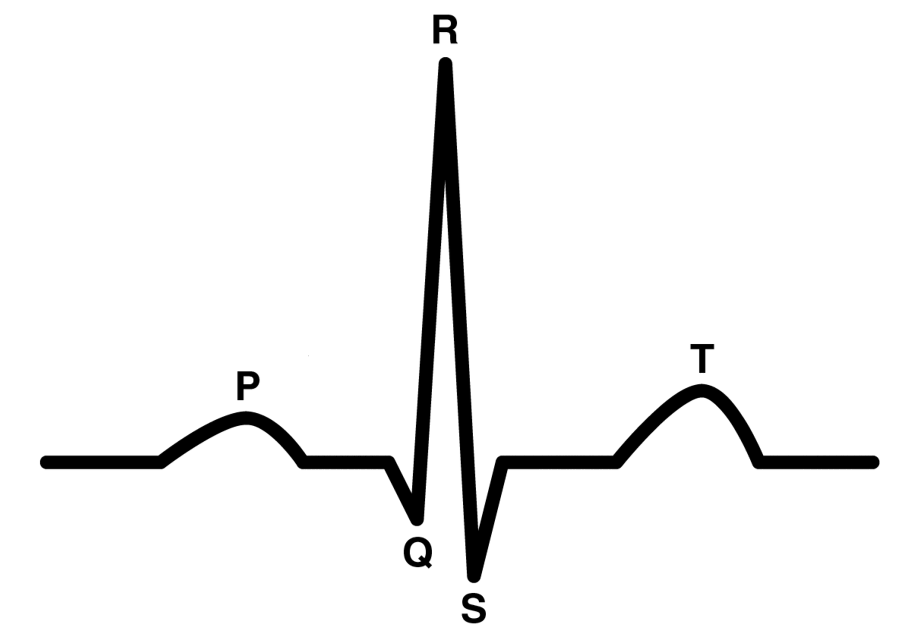
So, what do those waves mean? Well, let's label them so we can discuss each part of the wave individually:
Okay, now we can start finally start talking about the heart!

The heart beats like this:
1. the atria contract (these are the small chambers on the "top" of the heart)
2. the ventricles contract (these are the larger chambers on the "bottom" of the heart)
The blood flows like this:
1. de-oxygenated blood enters the right atrium
2. when the atrium contracts the blood is pumped into the right ventricle
3. when the right ventricle contracts the blood is pumped into the lungs and oxygenated there
4. the blood comes back from the lungs and enters the left atrium
5. when the left atrium contracts the blood is pumped into the left ventricle
6. when the left ventricle contracts, the oxygenated blood is pumped out to the whole body
The electrical activity of the heart flows like this:
1. the SA node is the "pacemaker of the heart" and is located in the right atrium, it fires and the atria both contract, this is the "P" wave as shown above.
2. the electrical impulse then travels through the center of the heart and down to the ventricles, when they contract you see the "Q","R", and "S" waves shown above.
3. the electrical impulse then re-polarizes or "resets" which creates the "T" wave shown above.
Interpreting abnormal ECG's:

Above we see a normal beat (a P, Q, R, S, and T), another normal wave, and then a long pause followed by a Q, R, S, T and then another normal beat. So, that 3rd set is preceded by a long pause and is also missing it's "P" wave. What does this mean?
The "P" is where the electrical activity starts. The SA node fires and the atria attract. There is an issue here. This didn't happen during this beat. When the ventricles don't get a signal to contract they wait for a little bit and then, rather than not beating at all, they'll fire on their own. So, the impulse to beat didn't happen so the ventricles fired on their own. This is called an "escape beat".

Above we see a T wave (the end of the previous beat), then a normal P, Q, R, S, T followed by a P-wave without a Q, R, S, and T. Then another P-wave all alone, then the next complex is normal (P, Q, R, S, and T). After that is another P-wave without a Q, R, S, and T, then 2 more normal complexes. What is happening here?
Well, when there is a P-wave that is not followed by a Q, R, and S you have an electrical signal that is firing the atria, but then not getting passed along to the ventricles to cause them to contract. This is called "heart block" -an appropriate name since the signal is getting blocked between the atria and ventricles somewhere in the middle of the heart!
The above is a very brief although only slightly simplified introduction to ECG's. For more information I highly recommend checking out: http://ekg.academy/ where they have lessons and lots of practice leads to nerd out on!
